
Fran Covington, age 82, has a history of cardiovascular disease, chronic diastolic heart failure, type 2 diabetes, and chronic obstructive pulmonary disease (COPD). She lives at home with her husband and enjoys gardening and visiting with her grandchildren.
Like Mrs. Covington, Myrna Wilson is age 82 with cardiovascular disease and a history of chronic diastolic heart failure, type 2 diabetes, and COPD. She lives in a skilled nursing facility and requires assistance with all routine daily activities. She complains of progressive physical decline and weakness and has lost 12 lb unintentionally in the past year.
Although these women are the same age with the same major comorbid conditions, one is active and independent while the other shows functional decline. What explains the striking difference between them? Most likely, the answer is frailty syndrome.
Distinctly different from general disability and multimorbidity, frailty syndrome is characterized by signs and symptoms common in patients identified as frail. The condition is linked to various comorbid conditions—specifically, cardiovascular and pulmonary diseases and diabetes.
Frailty syndrome remains underrecognized, even though it’s associated with functional decline and costly adverse health events in older adults, such as disability, hospitalization, falls, fractures, and deaths. It’s strongly linked to lack of resilience and decreased ability to adapt to physical stressors, as well as a higher risk of peri- and postoperative complications, including prolonged mechanical ventilation and longer stays after elective surgeries. Recent literature describes frailty as causing a domino effect because of the high potential for a cyclic cascade of adverse health-related events once an elderly adult becomes frail.
Epidemiology
Frailty is most common in adults older than age 70. Its prevalence rises substantially after age 80. Research indicates frailty is more common in elderly females, African- Americans, and persons with less education and of lower socioeconomic status.
Know that being frail isn’t synonymous with being thin or cachectic; nor is it as simple as the medical diagnosis of sarcopenia (muscle wasting). While simultaneous weight loss and muscle wasting commonly are correlated with frailty syndrome, obese persons (even, in some cases, the morbidly obese) can be frail. So when evaluating older adults for frailty syndrome, be sure to use a validated questionnaire (such as one of those described in this article).
Assessment
When asked to describe frailty syndrome, some clinicians might answer, “You know it when you see it.” But is this really true? In 2001, Fried, et al pioneered efforts to identify a clear, comprehensive definition of this previously ambiguous syndrome (some times known as failure to thrive). They identified major characteristics of frailty as unintentional weight loss of more than 10 lb within the last year, weakness, poor endurance, exhaustion, slow gait, and a selfreported feeling of exhaustion and low activity level. This landmark study generated an explosion of frailty literature. Since then, more evidence has surfaced suggesting such clinical characteristics as cognitive decline and an increased number of comorbid conditions are possible additional markers for frailty syndrome.
Screening and identification
While more research is needed on frailty syndrome, early identification and management are crucial. Yet no community-wide or population- based frailty screening recommendations exist. Although international consensus statements recommend screening every patient age 70 or older for frailty in every healthcare setting, such screening continues to be largely overlooked as a routine part of risk assessment for elderly adults across all healthcare settings. Consider, for example, the many screening tools in place for hospital admission to a medical-surgical floor: Elderly adults may be screened for physical and emotional abuse, alcohol use, tobacco use, depression, fall risk, and potential for impaired skin integrity. Yet few healthcare settings screen them for frailty.
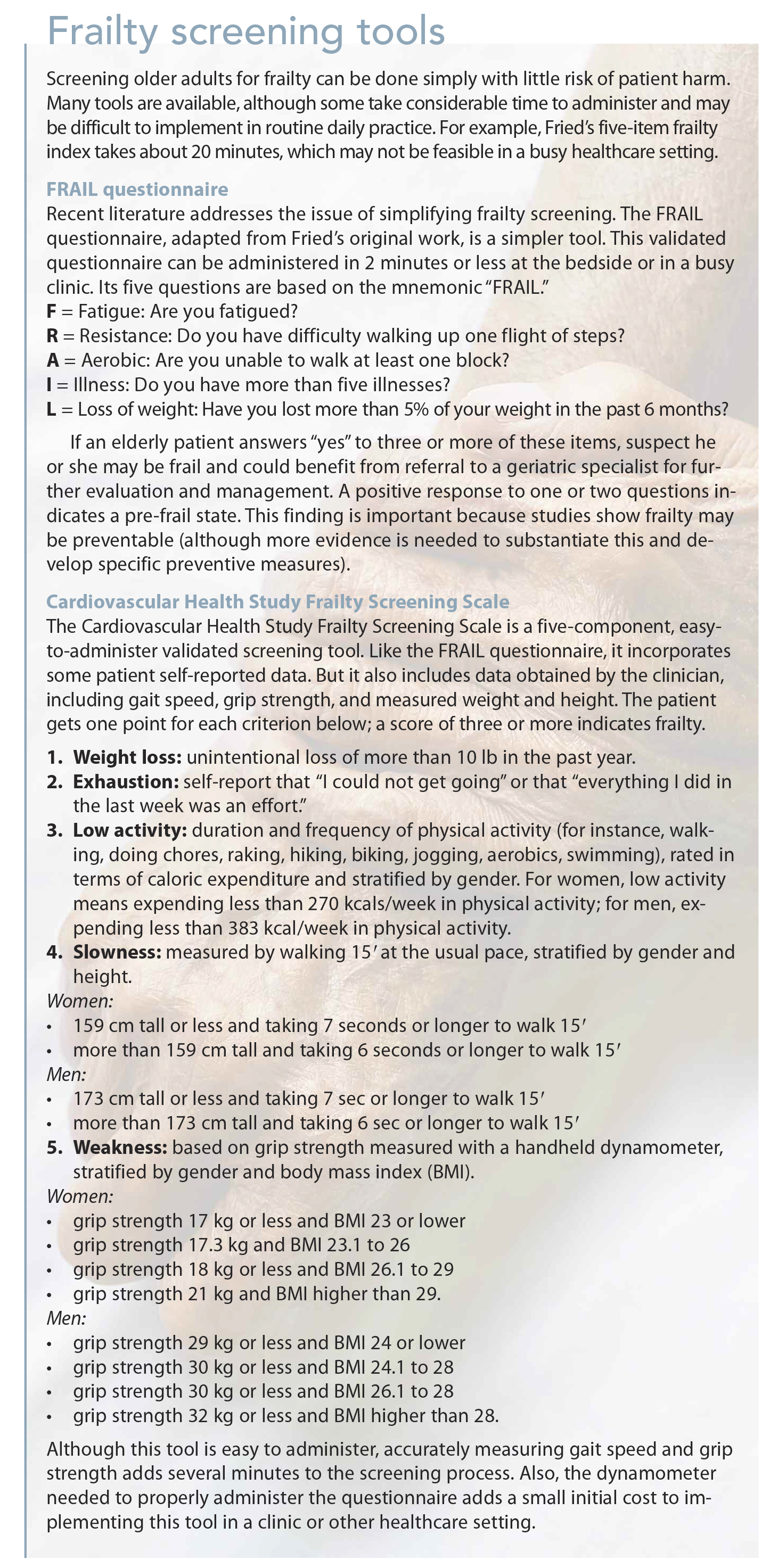
As a nurse, you can play a leading role in screening and identifying frail patients. This role presents a tremendous opportunity for every nurse who cares for older adults to have a meaningful impact on the quality of care for this vulnerable population. For information on screening tools for frailty syndrome, see Frailty screening tools.
Treatment and recommendations for clinical practice
Although frailty is strongly associated with advancing age, we know elderly adults can enjoy life in their ’80s,’90s, and beyond without becoming frail. Based on emerging evidence, a growing number of experts believe that with early identification, frailty syndrome probably can be treated and even prevented. However, this conclusion hasn’t been firmly substantiated by scientific evidence, highlighting the need for more studies on frailty prevention and treatment, including effective interventions for managing pre-frail and frail states in elderly patients.
Given the known adverse effects of frailty, clinicians should develop treatments and interventions aimed at improving the quality of life, reducing the need for institutionalization, and decreasing overall healthcare costs. In many cases, nonpharmacologic interventions, such as physical therapy and activity programs, are primary treatment strategies to diminish the major manifestations of frailty (such as sarcopenia and falls).
Treatments
In 2012, the majority of an international consensus group agreed that four potential treatments can be used to manage frailty in older adults:
• exercise
• nutritional and protein supplementation
• vitamin D supplements
• elimination of unnecessary medications.
Exercise programs are well supported as a way to reduce adverse health events associated with frailty, including falls and hospitalizations. Because weight loss is common in frail patients, nutritional and protein supplementation is recommended. Frail adults also should receive vitamin D supplements and reduce or eliminate unnecessary medications, as appropriate. We need further research to determine more specific or advanced treatments for frailty.
Improving elders’ outcomes
Frailty in older adults has become an increasingly important topic in the medical literature, and the importance of identifying frailty is well documented. What’s more, frailty has influenced care processes in our leading healthcare delivery systems.
As nurses, we’re well positioned to implement frailty screening in our daily clinical practice to improve the health outcomes of elderly patients and help develop the weight of evidence in favor of early identification of pre-frail and frail older adults. Nurses across all settings should become involved in screening, early identification, and management of this syndrome in elderly adults.
Kristi Phillips-Burkhart is the lead structural heart team coordinator at Mount Carmel Health System in Columbus, Ohio. (Names in the scenario are fictitious.)
Selected references
Dodds R, Sayer AA. Sarcopenia and frailty: new challenges for clinical practice. Clin Med (Lond.). 2015;15(suppl 6):s88-91.
Fried LP, Tangen CM, Walston J, et al; Cardiovascular Health Study Collaborative Research Group. Frailty in older adults: evidence for a phenotype. J Gerontol A Biol Sci Med Sci. 2001;56(3):M146-56.
Heuberger RA. The frailty syndrome: a comprehensive review. J Nutr Gerontol Geriatr. 2011;30(4):315-68.
Kim H, Higgins PA, Canaday DH, Burant CJ, Hornick TR. Frailty assessment in the geriatric outpatient clinic. Geriatr Gerontol Int. 2014;14(1):78-83.
Morley JE, Vellas B, van Kan GA, et al. Frailty consensus: a call to action. J Am Med Dir Assoc. 2013;14(6):392-7.
Woo J, Leung J, Morley JE. Comparison of frailty indicators based on clinical phenotype and the multiple deficit approach in predicting mortality and physical limitation. J Am Geriatr Soc. 2012;60(8):1478-86.
Xue QL. The frailty syndrome: definition and natural history. Clin Geriatr Med. 2011; 27(1):1-15.












{kind=link}