Bridging the education-to-practice gap.
Editor’s note: This is an early release of an article that will appear in the November 2021 issue of American Nurse Journal.
To read other articles in the Beyond the Pandemic series, click here.
Takeaways:
- An academic institution successfully developed and implemented a virtual low-burden, learner-driven interprofessional tool kit in the clinical learning environment.
- The pilot was successful in expanding virtual experiential interprofessional education offerings and learner/program engagement volume while adhering to best practices.
As the complexity of healthcare delivery increases, so does the demand for collaborative teams of health professionals with unique and complementary knowledge and skills. According to the World Health Organization, interprofessional collaborative practice occurs “when multiple health workers from different professional backgrounds work together with patients, families, carers, and communities.” This team approach was reinforced in the 2021 National Academies of Medicine consensus study report, The Future of Nursing 2020–2030: Charting a Path to Achieve Health Equity, which identified collaboration with other disciplines and sectors as a key factor in achieving priority outcomes that advance health equity and the nursing profession.
In line with this vision, the American Association of Colleges of Nursing 2021 Essentials: Core Competencies for Professional Nursing Education includes interprofessional partnerships as the sixth core competency domain. The four subcompetencies in the domain align with several Interprofessional Education Collaborative (IPEC) competencies. (See Essential alignment.)

This collaborative focus requires innovative interprofessional educational (IPE) curricula capable of preparing teamwork-ready health professionals. IPE experiences should be developmentally appropriate to the stage of the learner, integrated within the profession-specific curriculum, and they should continue over the course of the learner’s preprofessional education. This allows learners to form not only their profession-specific identity, but also their interprofessional identity as they’re socialized into, learn about, and then practice collaboration in the context of their uniprofessional education.
This article describes how an academic institution successfully developed and implemented a virtual low-burden, learner-driven interprofessional tool kit in the clinical learning environment.
Innovative curricula
The University of Minnesota launched its formal 1Health IPE program in 2009. The curriculum design progresses developmentally, from orientation to IPE (Phase I) to interprofessional knowledge and skills acquisition (Phase II), which prepares students for collaborative practice in experiential settings (Phase III.)
Program overview
The image below summarizes the University of Minnesota interprofessional education curriculum.
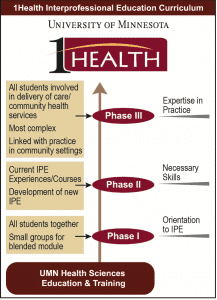
Phase I
Phase I has evolved from a multisession course offered across one term to a single 4-hour introductory IPE experience. In its current form, Phase I (Better Together) includes completion of a 1-hour independent online module, followed by a 3-hour synchronous session. Because over 1,400 learners from 21 programs are required to participate, they’re scheduled for one of six to seven sessions conducted within their first term.
Participants learn about values and the patient experience, engage in small interprofessional groups to explore communication styles and system-level effects of teamwork, and discover roles and responsibilities of health profession experts as they rotate through the groups. This is the only portion of the IPE curriculum that’s uniform across the professions.
Phase II
In Phase II, learners participate in various program- or self-selected interprofessional activities. Some experiences are facilitated by the university’s centralized IPE team, whereas others are implemented via direct program collaborations. Opportunities include interprofessional case competitions, simulations, client interviews and examinations, and online interactive modules with a beginner escape room.
All activities in this phase aim to build interprofessional skills in communication and teamwork and increase understanding of ethics and the roles and responsibilities of other professions. Most learners engage in one or more Phase II activities on either a required or voluntary basis.
Phase III
Phase III is the experiential portion of the longitudinal IPE curriculum, occurring toward the end of a learner’s education. Learners apply their acquired IPE skills in clinical and community settings while learning from practicing health professionals.
Although implemented in 2014, Phase III is the least developed. Until 2020, one centrally facilitated Phase III IPE was offered during full-time experiential placements, which consisted of an in-person session that included a guided reflection on interprofessional practice, a novel interprofessional escape room activity, and a debriefing. Participation has consistently included three professions—medicine, nursing, and pharmacy. Few additional program-facilitated Phase III IPE activities are available.
A priority goal for the 2020–2021 academic year was to expand Phase III offerings. Growth opportunities included increasing the number of experiential interprofessional activities offered, the overall volume of learners participating, and the number of health professions engaged in this phase.
Expanding experiential IPE
Two of the university’s three codirectors of interprofessional education were charged with developing and expanding Phase III. They also held faculty positions, one in the doctor of nursing practice (DNP) program and the other in the doctor of physical therapy (DPT) program.
The codirectors developed an IPE learner-driven toolkit that promotes and assesses interprofessional competency development in the experiential learning environment. All IPE activities are designed for a virtual environment. The initial toolkit consists of five discrete interprofessional activities: Get to Know Your P.A.L. (Peer Allied Learner—a learner from another profession), Find Your Interprofessional ‘Why’, Communication in Action, Teams in Action, and Contemporary Interprofessional Case Study. (See Toolkit activities.)
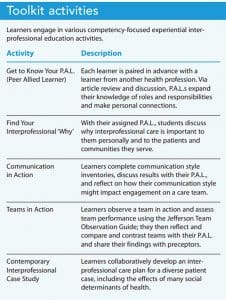
Each activity aligns with IPEC subcompetencies (communication, roles and responsibilities, teams and teamwork, and values and ethics) and the Essentials Domain 6 competencies. During full-time experiential placements, learners use a consistent activity format that includes independent prework, synchronous (virtual or in-person) IPE engagement with a paired interprofessional peer, a reflective submission, and an activity evaluation.
The toolkit provides structured opportunities for learners to engage in interprofessional activities during experiential placements. Because of the toolkit’s learner-driven design, IPE activities don’t require supervision or additional teaching time from clinical preceptors. The toolkit not only helps the learner see the interprofessional work that’s already happening around them, but also strengthens their own interprofessional practice skills.
Learner selection
Learner selection for the pilot initiative prioritized professions and locations typically not involved in Phase III. Access during the spring term was enhanced using a novel placement data analysis approach. In the past, sites with traditionally co-located learners from multiple professions had been identified primarily in metropolitan areas or in large cities or healthcare facilities. In the pilot, the new placement data analysis technique revealed 10 geographic clusters of experiential educational locations across rural Minnesota, in which learners from several professions were located within 1 hour of each other.
Learners were invited to engage with an assigned interprofessional P.A.L. from their cluster, promoting social interactions in rural environments. Previously, these learners couldn’t participate in campus-based IPE programming and few interprofessional learning opportunities were offered in the rural communities.
Professions without a history of Phase III engagement were selected for summer term participation. The codirectors engaged directly with experiential coordinators and program directors to design an approach that would meet program needs. The selected professional programs committed to embedding the IPE pilot activities as requirements in curricular coursework and included a standardized description in their syllabi. Administrative burden wasn’t added to the program director or experiential coordinator, but activity completion ultimately was required and reinforced by the programs.
The virtual design enabled geographically diverse P.A.L. placements to participate in the toolkit pilot. If convenient, learners were encouraged to connect in person. All materials were housed within a course in the university’s learning management system (the experiential learning interprofessional hub). Communication between the codirectors and the learners was conducted via email.
Outcomes
Pilot curriculum evaluation focused on Phase III growth (learner volume, increased offerings, and increased profession program participation) student perceptions, and resources required (including time commitment).
Learner volume
The pilot curriculum, delivered twice, has demonstrated positive growth. The first opportunity, in spring 2021, was offered to over 260 learners from 14 health profession programs on a voluntary basis near the end of their final academic placement. Four learners—two in the DNP program and two in the DPT program—participated.
The second opportunity, in summer 2021, was structured as an embedded requirement within three programs’ (medical laboratory sciences, doctor of occupational therapy, and speech language pathology) experiential coursework. Learner volumes from each program were 13, 18, and 26, respectively. Pharmacy learners also were invited to join, adding 6 participants for a total of 63 learners.
All learners completed three of the five IPE toolkit activities: Get to Know Your P.A.L., Find Your Interprofessional ‘Why’, and one additional activity. Assignments to the additional activities were distributed fairly evenly across learners (18 to Communication in Action, 26 to Teams in Action, and 23 to Contemporary Interprofessional Case Study).
Offerings and participating professions
Before this initiative, only three health profession programs participated regularly in the centrally offered Phase III activity as a required, embedded experience (medicine, nursing, and pharmacy). This original activity required learners to physically return to campus during full-time rotations, which wasn’t possible for many programs. The virtual element of the new experiential curriculum expanded accessibility by incorporating additional professions previously unable to participate.
In our pilot implementation, the number of professions participating in structured, required Phase III IPE curriculum doubled from three to six. More professional programs will be added to activities in the coming academic year.
Student perceptions
Phase III IPE participants were invited to evaluate the feasibility and acceptability of individual activities. The response rate ranged from 78% to 100% depending on the activity. In general, learner feedback was positive. Over 87% of respondents agreed or strongly agreed with the statement: “Regardless of my opinion of this specific experience, I believe that intentional interprofessional experiential opportunities should be designed and offered during clinical rotations.”
In open-ended comments, learners qualitatively reported that they desired engagement with their P.A.L. in person in clinical practice. They also rated activities lower if they didn’t envision themselves working directly with their paired profession in practice.
Resources
The primary resources needed for initial development of the experiential IPE curriculum were leadership faculty and staff time. The experiential IPE codirectors contributed a combined average of 8 to 10 hours per week over the course of 9 months, with approximately 2 hours per week of assorted staff assistance. Primary tasks included IPE activity development, evaluation planning, placement data analysis, program communications, and learning management system design. An interprofessional team of three student interns also contributed to the system design at a combined 3 hours per week over 9 months.
All technology platforms were supported by the university at no additional cost to the programs, and the virtual execution required no physical space or supplies. The codirectors managed the activities and took on IPE oversight responsibility from experiential coordinators and program directors. Given the learner-led design of activities, no burden was placed on clinicians or community organizations.
All of this developmental work can be viewed as an up-front investment, with modifications and additions to the curriculum over time as we build on this foundation. We perceive a high return on investment in this low-burden, high-impact approach to experiential IPE.
Lessons learned
A literature review by Abu-Rish and colleagues demonstrates that learner engagement in IPE experiences bridges the gap from education to collaborative practice. Although barriers (such as incompatible schedules, full curricula, lack of other health professionals to engage with) may exist, they can be overcome with persistence and innovation. Our experiential IPE toolkit pilot explored the feasibility, acceptability, and logistics of a learner-driven IPE curriculum. The pilot successfully expanded virtual experiential IPE offerings and learner/program engagement volume while adhering to best practices when creating a developmentally appropriate, longitudinal, integrated curriculum.
As with any pilot, many lessons were learned:
- Embed experiential IPE activities. Learner engagement in this pilot was greater when experiential IPE activities were embedded as requirements in academic curriculum coursework as compared to voluntary participation. Of note, lower learner participation in the voluntary spring pilot offering may have been partially attributable to the timing of a global pandemic and late recruitment close to learners’ graduation.
- Obtain full commitment from program leadership. Supportive reinforcement from experiential coordinators and program directors regarding IPE expectations was appreciated in the few instances where learners weren’t engaged in their activities. The standardized syllabus statement added by all programs for the IPE requirement provided the option to invoke an academic course consequence if warranted.
- Communicate with learners early and often. Learners are busy during full-time experiential placements and may intentionally delay or procrastinate completing requirements. Frequent email reminders and a sense of responsibility to their assigned interprofessional peer contribute to timely engagement.
- Ensure involved programs are appropriately represented. An interprofessional identity doesn’t replace individual professional pride. Learners expressed disappointment in the occasional incidence of perceived poor representation, including when one participating profession was temporarily missing from an evaluation tool dropdown list, when a posted video for one profession was more representative of a different profession, or when an interprofessional case didn’t have the desired authenticity for one profession.
- Harness technology to connect interprofessional learners. Traditional co-location isn’t required for learners to engage interprofessionally during full-time experiential placements. A shared set of activities conducted virtually and rooted in common interprofessional competencies promotes learner development. Geographic co-location and collaboration outside of one’s home organization or institution are effective options to expand the number of programs and learners involved.
Pursuing excellence
Next steps will focus on further expansion of experiential activity offerings, continued growth of health profession learner and program inclusion, and enhanced collaboration with community and clinical partners to determine mutually beneficial contributions. We look forward to pursuing excellence in interprofessional practice and education through academic-practice partnerships that improve the health of the communities we serve.
The authors are codirectors at the Center for Interprofessional Health, University of Minnesota in Minneapolis. Cheri Friedrich is a clinical professor in the school of nursing. Brian Sick is an associate professor in the medical school. Sara North is an assistant professor in the division of physical therapy in the medical school.
References
- Abu-Rish E, Kim S, Choe L, et al. Current trends in interprofessional education of health sciences students: A literature review. J Interprof Care. 2012;26(6):444-51. doi: 10.3109/13561820.2012.715604
- American Association of Colleges of Nursing. The Essentials: Core Competencies for Professional Nursing Education. 2021.
- Brandt BF. Update on the US National Center for Interprofessional Practice and Education. J Interprof Care. 2014;28(1):5-7. doi: 10.3109/13561820.2013.852365
- Health Professions Accreditors Collaborative. Guidance on Developing Quality Interprofessional Education for the Health Professions. February 1, 2019.
- Institute for Healthcare Improvement. Health equity.
- Interprofessional Education Collaborative. Core Competencies for Interprofessional Collaborative Practice: 2016 Update.
- Lawlis TR, Anson J, Greenfield D. Barriers and enablers that influence sustainable interprofessional education: A literature review. J Interprof Care. 2014;28(4):305-10. doi: 10.3109/13561820.2014.895977
- Lyons KJ, Giodano C, Speakman E, Smith K, Horowitz JA. Jefferson Teamwork Observation Guide (JTOG): An instrument to observe teamwork behaviors. J Allied Health. 2016;45(1):49-53.
- National Academies of Sciences, Engineering, and Medicine. The Future of Nursing 2020-2030: Charting a Path to Achieve Health Equity. Washington, DC: The National Academies Press; 2021.
- Sick BT, Hager KD, Uden DL, et al. Using a guided reflection tool and debriefing session to learn from interprofessional team interactions in clinical settings. J Interprof Educ Pract. 2019;14:53-7. doi: 10.1016/j.xjep.2018.11.007
- Weiss KB, Passiment M, Riordan L, Wagnber R. Achieving the Optimal Interprofessional Clinical Learning Environment: Proceedings from an NCICLE Symposium. National Collaborative for Improving the Clinical Learning Environment. January 18, 2019.
- World Health Organization. Framework for Action on Interprofessional Education & Collaborative Practice. 2010.